
Tuberculosis
The 19th century’s silent killer
By Valentin Charlier
What did Queen Louise d’Orléans, George Orwell, Frédéric Chopin, Franz Kafka, and Thérèse of Lisieux have in common? They all died from tuberculosis, the same disease that claimed millions of lives across the world. For centuries, tuberculosis was one of humanity’s deadliest companions, likely the leading cause of death in human history.
In Belgium, tuberculosis was a major killer until the early 20th century, particularly as urbanization and industrialization reshaped living conditions. But were all Belgians affected equally? Let’s explore how deaths from tuberculosis affected Belgium, and how it was eventually brought under control.
Image: Cristobal Rojas, La Miseria, 1886 – Oil on Canvas (© Galería de Arte Nacional, Caracas- Venezuela)
What is tuberculosis
What Is Tuberculosis
Tuberculosis is an infectious disease caused by the bacterium Mycobacterium tuberculosis. It primarily attacks the lungs, but can also spread to other organs. Typical symptoms include persistent coughing, fever, weight loss, and fatigue.
Where Does it Occur?
Tuberculosis is as old as civilization itself: traces of the disease have been found in ancient human remains. Throughout history, it thrived in crowded, unsanitary environments, and remains closely linked to poverty and poor living conditions.
Diagnosis and Treatment
The invention of the stethoscope and the chest-X-ray allowed diagnosis. Before antibiotics, treatment options were limited. Rest and nutritious food, were the main approaches. Everything changed in 1943, when antibiotics offered the first real cure.
Prevention and Control
Tuberculosis spreads easily in poor living conditions, so better housing and hygiene have helped reduce it. Still, drug-resistant strains are rising, and many people lack access to proper treatment.

History of tuberculosis
Tuberculosis is one of humanity’s oldest diseases, with evidence of infection dating back to the Neolithic period and written descriptions in ancient civilizations such as Egypt, India, and Greece. Because it slowly wastes the body, it was historically known as phthisis or “consumption.” For centuries, its cause remained unknown and was often attributed to hereditary weakness or imbalances in bodily humours.
The disease became a major public health threat in early 19th-century Western Europe during the Industrial Revolution. It thrived in overcrowded and unsanitary urban environments marked by poor housing, inadequate sanitation, and malnutrition. Around 1850, tuberculosis was the leading cause of death in many industrialized countries, accounting for 15–20% of all deaths.
In Belgium, infectious diseases caused approximately 40% of all deaths in 1851, with tuberculosis claiming more lives (18,72%) than any other endemic diseases like pneumonia( 4,09%), enteritis (4,08%) and whooping cough (2,93%) and remaining an important cause of death well into the twentieth century (Figure 1).
A modern understanding of tuberculosis emerged in the late 19th century when it was shown to be contagious in 1865 by Jean-Antoine Villemin, and when Robert Koch identified Mycobacterium tuberculosis as the causative agent in 1882. This discovery led to public hygiene measures and the isolation of patients in sanatoria, which played a key role in reducing transmission.
Click the disease names to include or exclude them from the graph.
Figure 1: Percentage of deaths due to major infectious diseases in Belgium (1851 - 1978)
Sources : Statistique générale de la Belgique : exposé de la situation du royaume (période décennalle de 1851-1860; 1861-1875 ; 1876-1900) publié par Ie Ministre de I’Intérieur et de I’Instruction publique. Brussel, 1864 ; 1885 ; 1907-1912. Statistique de la Belgique, Documents statistiques publiés par le Département de l’Intérieur avec le concours de la Commission centrale de Statistique, Bruxelles, 1857-1869. Annuaire statistique de la Belgique (1870-1978), publié par Ie Ministre de I’Intérieur et de I’Instruction publique. Brussel. Calculations by V. Charlier.
Figure 2: ?
Following the discovery of the contagious character of Tuberculosis B, control and prevention focused on improving living conditions, nutrition, sanitation, and the sanatoria. Throughout the first half of the 20th century, sanatoria became a cornerstone of tuberculosis control, offering spaces for prolonged care while physically separating infectious patients from the general population.
The vaccine Bacille-Calmette-Guérin was elaborated in the early 20th century and declared safe by the League of Nations in 1928. In Belgium, vaccination efforts were limited by medical scepticism and the absence of systematic programs. Antibiotics treatments became available in 1947, the last addition to the control arsenal. By then the decline in deaths attributed to TB was already well on its way thanks to the other interventions and changes in living conditions. The decline of tuberculosis has also been partly attributed to increased population resistance over time.
Despite the impact of antibiotics, the role of social determinants in tuberculosis cannot be overlooked, particularly poverty, housing conditions, and nutrition. In fact, the decline in tuberculosis mortality began before the widespread use of effective vaccines and antibiotics. Improvements in living and working conditions, hygiene, isolation and prevention measures, as well as increases in life expectancy at birth contributed significantly to the reduction in mortality from infectious diseases, a trend that was later accelerated by medical advances. However, more recent epidemiological patterns highlight additional risk factors, including HIV, diabetes, substance abuse, and smoking, alongside persistent poverty and limited access to effective treatment.
From killing 1 in 5, to nearly disappearing
Let us take a closer look at the evolution of tuberculosis through time in Belgium (Figure 3). The government started counting causes of death nationwide from 1851 onwards. That first year, tuberculosis killed 17,730 people, mortality from tuberculosis accounted for nearly 20% of all deaths or 1 in 5 of all deaths. Tuberculosis mortality peaked at 19,478 deaths in 1865.
Industrialization played an important role. In Belgium in the 1840s, many people migrated to urban areas, fleeing rural poverty and seeking better opportunities. The cities became overcrowded, with poor housing, unsanitary living conditions and poor nutrition forming an ideal ground for the disease to spread.
In 1866, Belgium was struck by a cholera epidemic, causing a drop in tuberculosis mortality. The high mortality caused by cholera reduced the pool of individuals susceptible to dying from tuberculosis. Living conditions at that time were extremely harsh, and populations were simultaneously exposed to multiple life-threatening infectious diseases, meaning that mortality was often determined by which infection occurred first rather than by a single underlying vulnerability.
In the decades after 1870, tuberculosis mortality began to decline. Improvements in nutrition, living and working conditions, public health and sanitation interventions, and a better understanding of disease transmission were key factors driving this decline.
Figure 3: Mortality from Tuberculosis from 1851 until 1978
Sources: Statistique générale de la Belgique : exposé de la situation du royaume (période décennalle de 1851-1860; 1861-1875 ; 1876-1900) publié par Ie Ministre de I’Intérieur et de I’Instruction publique. Brussel, 1864 ; 1885 ; 1907-1912. Statistique de la Belgique, Documents statistiques publiés par le Département de l’Intérieur avec le concours de la Commission centrale de Statistique, Bruxelles, 1857-1869. Annuaire statistique de la Belgique (1870-1978), publié par Ie Ministre de I’Intérieur et de I’Instruction publique. Brussel. Calculations by V. Charlier.
Data before 1903 should be interpreted with caution, as the diagnostic category used likely overestimated tuberculosis-attributed deaths. Misclassification was a common issue before the 19th century, especially among diseases which share common symptoms like respiratory diseases. The discovery of the pathogen by Robert Koch was key to understand and identify tuberculosis. In that sense, the sharp drop in deaths in 1903 was mainly due to the introduction of the first International Classification of Diseases in Belgium. Before 1903, tuberculosis was often recorded within the broad category “Phthisis and other chronic diseases.” The new classification separated tuberculosis from other respiratory diseases, leading to a break in the statistical series rather than a genuine decline in mortality.
During the 20th century, the disease declined steadily and only flared up during the two World Wars. The disorganization of everyday life, destruction, requisition of the healthcare institutions, overcrowding due to civilian and troop movements, food rationing, and a lack of hygiene, led to increased precarity and temporary rises in tuberculosis mortality Still, mortality due to TB continued to decline. In 1978, the number of people killed by tuberculosis was only 296, less than 1% of all deaths in Belgium.
Today, the yearly number of cases of tuberculosis is estimated by WHO at 10.9 million, and an estimated 1.09 million people died from it, mainly in South-East Asia and Africa. Many TB patients today live in regions where the public health system struggles to diagnose patients and organize treatment for multi-resistant tuberculosis. Antibiotic treatment can last for months and needs to be accompanied by adequate nutrition, which can be a major challenge for impoverished populations.
Figure 4: ?
A disease of industrial regions?
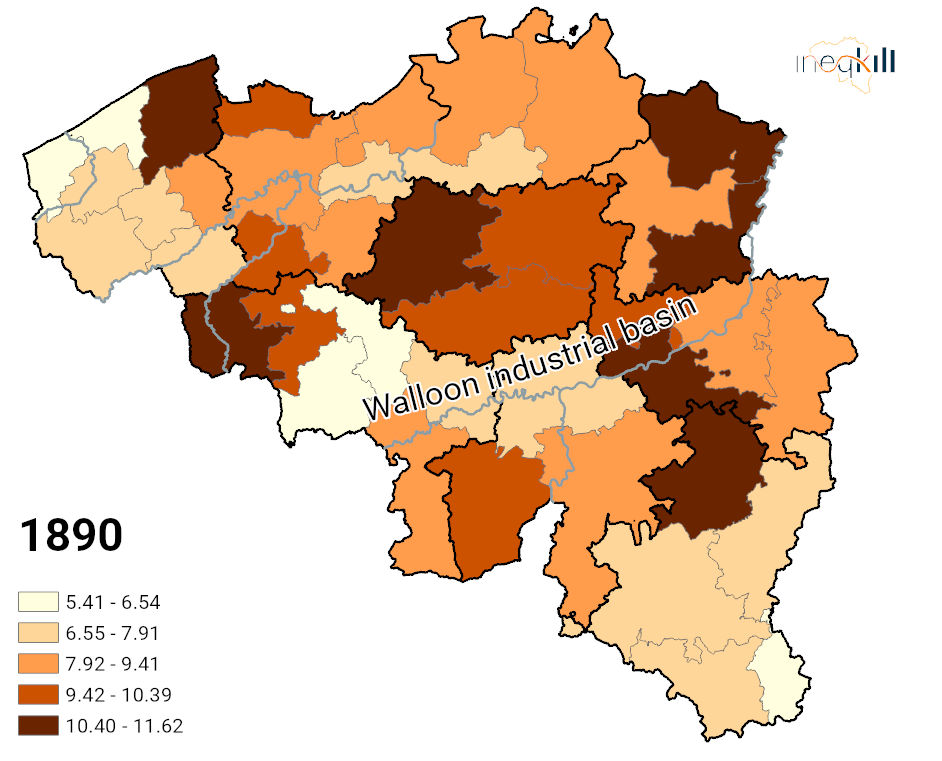
In the late 19th century (Map of 1890), relatively high mortality levels is are observed across the territory, with no single dominant cluster. Some urban districts such as Bruges, Brussels, and Leuven do however exhibit higher mortality rates. Urban environments were characterised by poor living conditions, including inadequate access to drinking water and sanitation systems, waste accumulation, and stagnant water, all of which created favourable conditions for the transmission of infectious diseases.
In Flanders, high tuberculosis mortality was not limited to industrial areas but also affected poorer agricultural regions, particularly in Limburg (e.g. Tongeren and Hasselt). This pattern can be linked to the agricultural crisis and the collapse of the domestic textile industry following the influx of cheaper industrial products in the 1840s and 1850s, which led to widespread rural impoverishment. Additionally, lower breastfeeding rates may have weakened immunity, increasing susceptibility to infection and contributing to poorer health conditions.
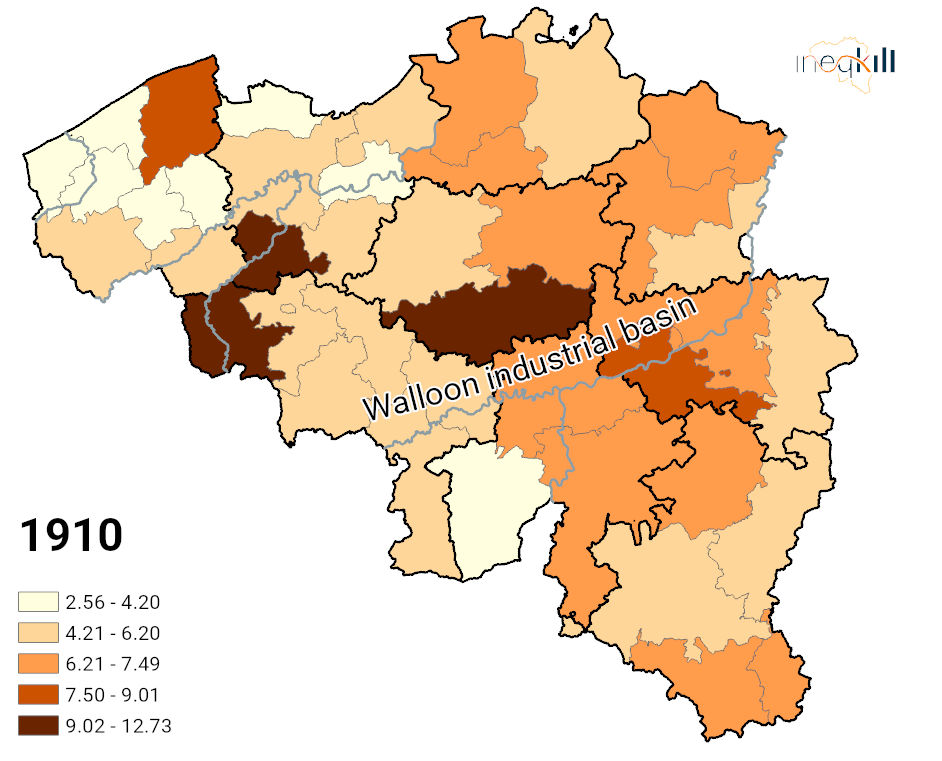
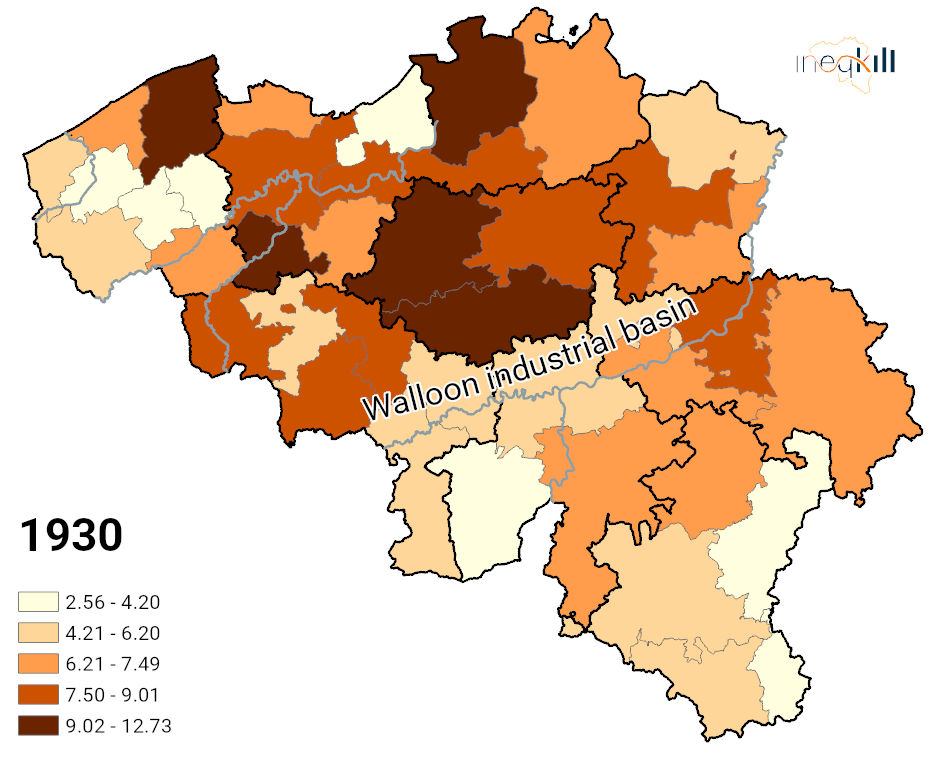
In the early 20th century (Map of 1910), mortality levels begin to decline, and spatial contrasts become less pronounced. High values become exceptional and more localised, while a larger share of the districts falls into intermediate or lower categories. This trend continues after World War I (Map of 1930) where the spatial distribution of TB mortality appears to be reconfigured: some districts that previously exhibited high mortality show improvement, while others retain relatively elevated levels.
Figure 5: Mortality related to tuberculosis from 1890 to 1950 (%)
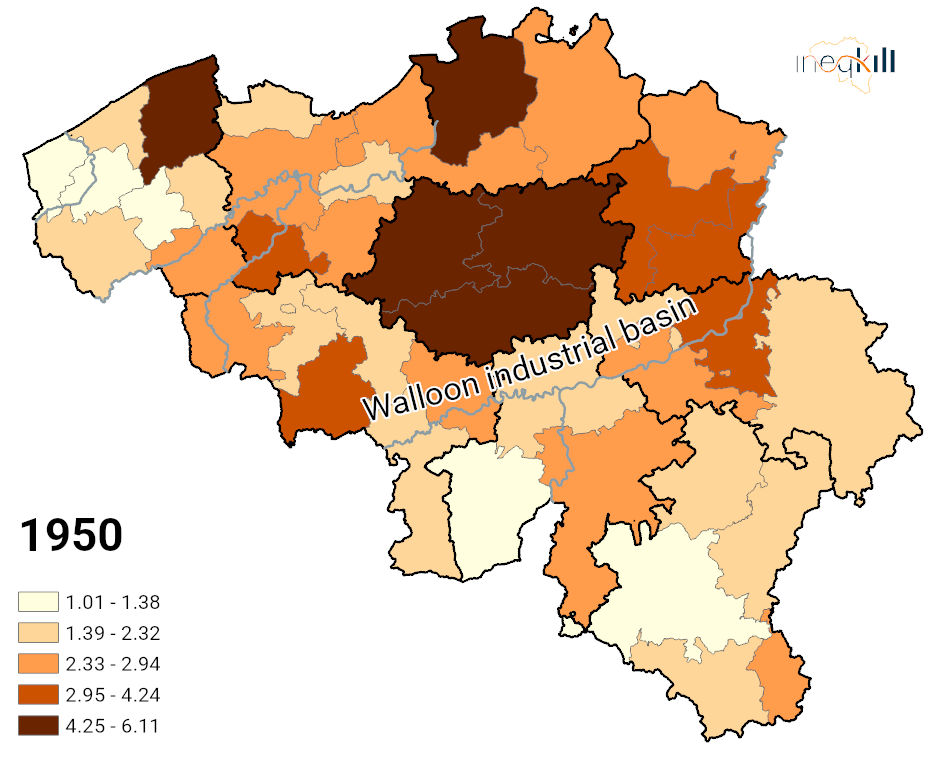
Sources: Algemeen Rijksarchief Brussel, Archief van het Nationaal Instituut voor de Statistiek: beweging van de burgerlijke stand en loop der bevolking, 1841-1976
The higher tuberculosis mortality in 1910 and 1930 observed in some districts such as Antwerp, Brugge, Brussel and Liège could also be related to the presence of sanatoria. Sanatoria were places where tuberculosis patients could stay to try to fight the disease with rest, clean air and better food (Figure 4). Isolation and rest were the main therapies during the 19th and early 20th centuries; an approach that remained important even after antibiotics entered the stage.
After World War II (map of 1950), tuberculosis mortality is substantially lower overall but unevenly distributed. Higher levels persist in several urban districts in Flanders (Bruges, Antwerp, Brussels, Leuven, and Hasselt) and become increasingly concentrated in areas with a mining and industrial past, such as Charleroi, Liège, and Mons. At this time, Wallonia entered a phase of economic decline following the collapse of heavy industry, accompanied by a deterioration in the health of industrial and mining workers. This was partly driven by worsening working conditions and exposure to lung-damaging technologies, such as jackhammers, which generated large amounts of fine dust.
From 1890 to 1950, the district of Bruges consistently showed higher tuberculosis mortality rates than other districts. This pattern can be explained by the late implementation of large-scale sanitation at the end of the 19th century, as well as by elevated mortality among young girls, related to the working and living conditions of women in the lace industry.
Figure 6: View of the Elisabeth sanatorium in Sijsele in 1932

The changing profile of tuberculosis victims
When we look at the people who died of tuberculosis through time, who stands out? And does their profile change over time or through space? How did inequality evolve?
When it comes to tuberculosis, men and women both had cause for concern, though for different reasons over time. Many forms of male employment were particularly unfavourable to lung health, especially in mining and industrial occupations (Figure 7), a pattern that became increasingly visible in the second half of the 20th century, when tuberculosis mortality predominantly affected men, notably in the industrial areas of Wallonia.
In contrast, during the 19th century and into the early 20th century, women were more socially disadvantaged, and their health may have suffered accordingly. Young girls in particular showed a greater vulnerability to tuberculosis, a susceptibility that may be linked to their disadvantaged position in society: they might have had less access to nutrition and healthcare, suffered the physical load of pregnancy, and, in some regions such as Flanders they were often employed in textile industries where they worked in poorly ventilated spaces, earned low wages and suffered widespread malnutrition.
Figure 7: Return of the miners by Constantin Meunier

Over time, the age groups most affected by tuberculosis also changed. From 1935 to 1950, individuals aged 15 to 54 bore the heaviest burden of tuberculosis mortality. After 1945, mortality from tuberculosis progressively shifted to older age groups, and by 1950 most deaths occurred among the elderly. This trend reflects both the improved health of younger individuals and population ageing. As the proportion of elderly individuals increased, tuberculosis mortality became increasingly concentrated in older age groups. It may also result from changes in the working environment, where deteriorating working conditions and prolonged exposure to occupational hazards increasingly affected an ageing workforce, making workers more vulnerable to respiratory diseases.
Deaths from tuberculosis are driven by poverty and industrialisation. However, further dimensions of disadvantage must be considered, such as the position in society.
Tuberculosis was once the leading cause of death in Europe and a defining feature of 19th century urban life. Its decline, driven by better living conditions, public health reform, and scientific discovery, marks one of humanity’s great public health successes.
Today, tuberculosis continues to thrive where poverty, overcrowding, and limited healthcare persist. Understanding its history reminds us how deeply health is shaped by social and economic conditions, and how progress against disease depends not only on medicine, but also on equity.
Our publications
- Charlier, V., Devos, I., Eggerickx, T., & Vanwambeke, S. O. (2024). The geography of tuberculosis mortality in Belgium between 1889 and 1991: A descriptive analysis. Espace Populations Sociétés, 2023/3-2024/1. https://doi.org/10.4000/12tpr
- Eggerickx, T., Sanderson, J.-P., & Vandeschrick, C. (2020), Mortality in Belgium from nineteenth century to today, Quetelet Journal, 8(2), 7‑59. https://doi.org/10.14428/rqj2020.08.02.01
- Eggerickx, T. & Tabutin, D. (1994), « La surmortalité des filles en Belgique vers 1890 », Population, 3, pp. 657-684, https://doi.org/10.2307/1533962
- Devos, I. (1996), La régionalisation de la surmortalité des jeunes filles en Belgique entre 1890 et 1910, Annales de démographie historique, 1996(1), 375‑407. https://doi.org/10.3406/adh.1996.1928
- Devos, I. (2006), Allemaal beestjes. Mortaliteit en Morbiditeit in Vlaanderen, 18de-20ste eeuw (p. 262), Academia Press.
- Devos, I., & Van Rossem, T. (2015). URBAN HEALTH PENALTIES. Journal of Belgian History/Revue Belge d’Histoire Contemporaine, 45(4).
Further Reading
- Davies, P. D. O. (2005), Risk factors for tuberculosis, Monaldi Archives for Chest Disease, 63(1), –. https://doi.org/10.4081/monaldi.2005.656.
- Deligne, C. (2016). Industrialisation, manure and water quality in the 19th century. The Senne River in Brussels as a case study. Water History, 8(3), 235‑255. https://doi.org/10.1007/s12685-016-0163-0
- Dyd, C., Lönnroth, K., Jaramillo, E., Williams, B., & Raviglione, M. (2009), Trends in tuberculosis incidence and their determinants in 134 countries, Bulletin of the World Health Organization, 87(9), 683‑691. https://doi.org/10.2471/BLT.08.058453
- Glaziou, P., Floyd, K., & Raviglione, M. (2018), Trends in tuberculosis in the UK, Thorax, 73(8), 702‑703. https://doi.org/10.1136/thoraxjnl-2018-211537.
- Mackenbach, J. P. (2020), A history of population health: Rise and fall of disease in Europe, Brill | Rodopi.
- Van Helden, P. D. (2003), The economic divide and tuberculosis: Tuberculosis is not just a medical problem, but also a problem of social inequality and poverty, EMBO Reports, 4(S1). https://doi.org/10.1038/sj.embor.embor842
- Wanlin, M. (2018). Tuberculosis in Belgium before, during, and after World War II. In Progress in Respiratory Research (pp. 144–151). S. Karger AG. https://doi.org/10.1159/000481482
- https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/global-tuberculosis-report-2024/tb-disease-burden/1-2-tb-mortality
Sources
- Algemeen Rijksarchief Brussel, Archief van het Nationaal Instituut voor de Statistiek: beweging van de burgerlijke stand en loop der bevolking, 1841-1976
- Statistique générale de la Belgique : exposé de la situation du royaume (période décennalle de 1851-1860; 1861-1875 ; 1876-1900) publié par Ie Ministre de I’Intérieur et de I’Instruction publique. Brussel, 1864 ; 1885 ; 1907-1912.
- Statistique de la Belgique, Documents statistiques publiés par le Département de l’Intérieur avec le concours de la Commission centrale de Statistique, Bruxelles, 1857-1869. Annuaire statistique de la Belgique (1870-1978), publié par par Ie Ministre de I’Intérieur et de I’Instruction publique. Brussel.
The Ineqkill Atlas of Mortality Inequalities in Belgium provides detailed information about mortality and diseases in Belgium from 1820 to 2025.
About
- Ineqkill Research Project
- Mission Statement
- Team
- FAQ's
Vrije Universiteit Brussel
Pleinlaan 5 (Room 2.17)
1050 Brussels, Belgium
e-mail: sylvie.gadeyne@vub.be

