
What is INEQKILL?
INEQKILL is a four-year interdisciplinary research project (2022-2026) that focused on a crucial dimension of inequality in society, the disparity in death, coined ‘ultimate inequality’. How inequality kills.
The COVID-19 pandemic incited renewed interest into infectious diseases as potential drivers of social and spatial mortality inequalities, alongside life-style disease (cardiovascular diseases and cancer) and external causes of death.
The project aims at generating new knowledge and insights into the origin and development of inequalities in all-cause and cause-specific mortality in Belgium. It tackles the long-term evolution of mortality inequalities (1800-2025) using an interdisciplinary approach based on expertise from demography, social epidemiology, medical geography and socioeconomic history.
INEQKILL addresses the following questions concerning how inequality kills:
- How have social and spatial differences in cause-specific mortality evolved in the context of rising living standards, improved social security and medical progress?
- How did these mortality patterns vary according to age, gender and migration status? And which factors can explain these?
Besides using Belgium’s rich and unique statistical heritage, the project takes advantage of state-of-the-art geographic information systems and statistical techniques. Integrating micro and macro level data, linking past and present, and engaging with the wider public, INEQKILL embodies a major and original initiative in enhancing our understanding of mortality inequalities in Belgium and beyond.
INEQKILL started in October 2022 and is an EOS (Excellence Of Science) Project financed by the Research Foundation – Flanders (FWO) and Fonds National de la Recherche Scientifique (FNRS). It is a collaboration between Interface Demography (Vrije Universiteit Brussel), Quetelet Center for Quantitative Historical Research (Ghent University), Center for Demographic Research (Université Catholique de Louvain) and Earth and Life Institute (Université Catholique de Louvain).
Project
The main objective of INEQKILL is to analyse social and spatial differences in all-cause and cause-specific mortality in Belgium between 1800 and 2025. The timing of the epidemiologic transition in Belgium is well known (see graph 1), but we do not know how this transition occurred and varied by social groups and areas.
- How did social and spatial inequalities in mortality evolve in the context of industrialisation, tertiarization, rising living standards, improved social security and medical progress?
- What were the effects of economic crises, epidemics and the world wars?
- How did these patterns vary according to age, gender and migration status? What factors at the individual household and local-regional levels can explain these differences?
In line with the (extended) fundamental cause theory by Clouston et al. (2016, 2021), we assume that social and spatial inequalities in mortality evolve
- according to the rise and fall of diseases (Mackenbach 2020), but
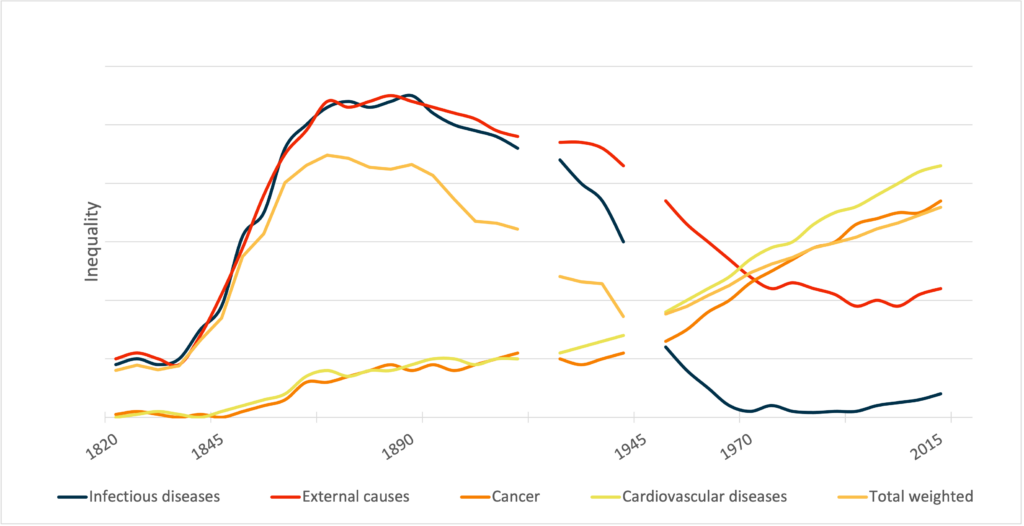
- depending on the local-regional and historical context. We assume that before 1945, industrial development followed by social and public health interventions had the greatest impact on the mortality of lower SES groups (from divergence to convergence), whereas after 1945 medical progress became the driving force behind the mortality decline, disproportionally beneficial for higher SES groups (from convergence to divergence)(see graph 2).
In other words, for INEQKILL the extended the fundamental cause theory applies not only to the top of the social scale, but also to the bottom.

The project consisted of 5 workpackages

WP1 assesses associations over space and time between cause-of-death mortality and socioeconomic, demographic and ecological variables, at the municipality level, the aggregated spatial unit maximizing demographic diversity and the spatial distribution of high, medium and low mortality.
- Were causes of death (infectious diseases, external causes, cancer, cardiovascular diseases, and emerging diseases) evenly distributed across Belgium?
- Where were men, women and children most and least vulnerable?
- Did spatial disparities increase or decrease between the early 19th century and today following INEQKILL’s hypotheses?
- How were spatial disparities in the causes of death related to local and regional living conditions, and to migration?

WP2 aims at analysing SE inequalities in all-cause and cause-specific mortality at the individual level over time. By examining four municipalities with very distinct societal contexts and exceptional sources (two in Flanders, two in Wallonia), we will relate the epidemiological transition to SES and the local context.
We focus on:
- Antwerp (a major international port),
- Zele (a small rural town where agriculture and textile production were important),
- Châtelet (a coal-mining town) and
- Cerfontaine (a rural village with few economic and institutional safety nets).
Were mortality inequalities stronger in an international port than in an industrial town or rural village? How did this differ by age, cohort, sex, and migration status? In line with INEQKILL’s hypotheses, how did inequalities in mortality converge or diverge? And what do the results tell us about the impact of industrialization?

WP3 focuses on the recent evolution of SE inequalities in mortality since the 1970s until 2025. It will enhance our understanding of the mechanisms at play by integrating micro and macro covariates of mortality.
The present-day data allow for very detailed and fine-grid analyses regarding (specific) causes of death, populations groups and covariates.
- How do SE inequalities in mortality evolve since the 1970s in the context of growing neo-liberalism and a declining impact of the welfare state?
- Can we link this evolution to the rise and fall of disease; do we observe smaller inequalities for declining diseases and growing inequalities for new or rising diseases such as COVID-19?
- What is the impact of contextual SE and environmental characteristics on mortality?
- How are individual mortality inequalities affected by macro characteristics?
- What is the role of migrant background? Do we observe comparable inequality trends in migrant populations as compared to the native population?
- And what can we learn from this in terms of inequalities in epidemiological transitions?

In WP4 we will create a central INEQKILL data infrastructure, storing and integrating the GIS and the data collected, linked and used in WP1, 2 and 3, as well as allowing their continuous update and consultation by each partner during the project. Regular backups will be assured. For each new dataset created, we will compile the appropriate metadata. For INEQKILL, the quality of the data, the reliability of the statistical analyses as well as the reproducibility and replicability of the methods are crucial.

WP5 will bring together and synthesize the results of WP1, WP 2 and WP3. It will address the implications of our results for the revised FCT theory of Clouston et al. (2016), confirming or refuting its main hypothesis, through systematic comparisons of the effects of socioeconomic inequality on mortality over time.
WP5 will confront results with our hypotheses and depict the evolution of social inequalities in mortality at the macro and micro levels in Belgium since the early 19th century. Given the long timeframe and the various local contexts covered, the variety of individual and contextual characteristics integrated and the focus on causes of death, WP5 will identify which new insights INEQKILL offers on the evolution of inequalities during the two centuries.
Which causes of death show the strongest and the weakest social gradients? How does this vary across time and place? And how do our results compare with the long-term international studies of social inequalities in mortality.